The removal of bodily autonomy from such a large part of the population has brought additional issues to a head and the reality is that our struggle must go beyond abortion to address the issues of bodily autonomy and reproductive rights.
The recent case of the 10 year old Ohioan girl that was raped who could not get an abortion in Ohio and had to go to Indiana to get an abortion has brought up a number of issues around bodily autonomy that need to be discussed.
The current discussion around this case is appalling. Disgusting comments from right-wing politicians and the media included the denial of her existence and evidence of the situation by Jim Jordan, the denial of the case being reported to the police by the Ohio Attorney General Dave Yost, a tweet from the South Dakota Governor Kristi Noem arguing that it was a fake story, refusals to accept the fact that a 10 year old could get pregnant and accusations against the doctor that diagnosed the pregnancy and rape and the doctor that performed the abortion in Indiana. Then, came the arrest of Gerson Fuentes for the rape who confessed to raping her twice. This led to questions about his “immigration status” because they had not said enough stupidity and of course where would they be without accusing all migrants of being rapists? Biden was “shocked” that a rape victim couldn’t get an abortion (and a child rape victim at that) and concentrated on the circumstances responsible for a 10 year old being pregnant and the additional stress of her having to leave the state to get an abortion.
There are so many things wrong with how a nation-wide debate on women’s bodily autonomy is used to discuss the specific issue of a 10 year old rape victim, that, quite frankly, it is shocking. Part of the issue is the medical ignorance of so many right-wing (politicians and those politically on the right) in the US. In November 2019 the Ohio state legislature passed a law requiring the reimplantation of ectopic pregnancies in the uterus or face charges of “abortion murder.” The fact that this is medically impossible seems irrelevant to the Ohio legislature, the only thing that is important is the sanctity of human zygotes, not the ability of the doctors to actually do their jobs to protect a women’s lives (you can die from an ectopic pregnancy after all).
The creation of the crime of “abortion murder” and “aggravated abortion murder” in Ohio is based on the idea that a fertilised egg must be treated as a “child.” Given that not even the Catholic Church (which maintains the sanctity of the foetus over the women incubating it) holds the view that the removal of an ectopic pregnancy is an abortion as the zygote is not viable. But Ohio’s Republicans, so concerned with the elimination of women’s bodily autonomy, abandon both medical science and even ridiculous Catholic doctrine to go further. The fact that this young rape victim could not get an abortion is due to laws passed in Ohio whose sole purpose is to remove control over people’s bodies from themselves.
The concentration on the rape (by Biden, for example) also nullifies her right to bodily autonomy. Of course, a rape is by definition a violation of the victim’s bodily autonomy. It is only because of the repulsive Hyde amendment that the manner in which a person becomes pregnant is of any import. The danger of forcing those that have been raped to go to the police in order to obtain an abortion if you find yourself pregnant is appalling. Convictions for rape are rare, the victim is subjected to appalling violations of their privacy and accusations of misconduct, their actions are questioned as though somehow, they, rather than the rapist, are the criminal.
The misogyny prevalent in our society as a whole is mirrored by the misogyny so often experienced in dealing with the police and criminal justice system. We can see this in the case of sexual harassment, sexual assault, and domestic violence complaints. It is not only misogyny; racism, homophobia, and transphobia are also endemic among the police and within the criminal justice system.
The case of the murdered sisters Bibaa Henry and Nicole Smallman is a case in point. The police refused to investigate the case when they didn’t return from Henry’s birthday party. The family found their bodies and reported it to the police. The police at the crime scene took grotesque selfies with their bodies and shared them with other police: “two dead birds” they called them.
Given the treatment of women, people of colour, disabled and LGBT+ by the police and criminal justice system, reporting a crime of this nature exposes you to further violations. Then there is also the social and cultural shame which is also misogynistic as though “good” girls don’t get sexually assaulted and raped. Since this is a societal and cultural issue, even if we know that this is accusation is false, we are still repeatedly told this. So on top of the rape and sexual assaults we have the shame of this happening to us; it is not rational, but this comes from the societies we live in. Many victims of sexual assault and rape simply do not want to report this to the police. But if you are required to report a rape to get an abortion in your state, then you have to again go through the violation against you, this time by the state (along with your family and culture).
Given how common sexual assault is and how difficult it is to deal with the police on this issue, no one should be forced to go to the police. Yes, that makes prosecution of the rapists and assaulters extremely difficult, but what needs to change is the misogyny and shaming and blaming of the victims of sexual assault and rape.
Returning tothe Hyde Amendment, I have never quite understood the incest qualification for the Hyde Amendment. If it is an adult relative and a child, this would be rape. If it is two related consenting adults, why would an abortion be covered by the state? I always wondered if this had something to do with eugenics (in its history, the US has had a long infatuation with eugenics after all; but maybe it is a presupposition that this happens always among poor people who could not afford an abortion otherwise? We do know that incest is not only done by the poor, so who knows?!
Then, of course, there is the life of the mother. That can be interpreted narrowly and broadly. It is narrowest interpretation; we are simply talking about the mother dying in pregnancy or during birth. If you have an ectopic pregnancy, will doctors have to wait until the fallopian tube ruptures and you are haemorrhaging to death to remove the embryo? Will they have to wait until it is clear that you are going to die to remove the foetus? If the foetus dies while in utero, will you have to wait until an arbitrary delivery time facing septicaemia?
In January 2022 in Poland, a woman known as Agnieszka T, who was carrying twins had to wait to get the first dead foetus removed, then when the second foetus died, they waited as well. She died because of a law in place that prohibited abortion unless the mother’s life was in danger. She and her husband wanted to get the foetuses aborted, that didn’t matter and now she is dead … leaving behind 3 living children and her husband.
The attempt by the Polish government to set up a registry of pregnancies and miscarriages following an almost total abortion ban bodes ill … I will not be surprised at all if this happens in US states that ban abortions as it will make it so much easier to keep track of who’s pregnant and who’s not … this will also clearly impact maternal health care as people will be frightened of prosecution if they have a miscarriage.
In a broader interpretation of the life of the mother, the issues of a future life, mental health, physical health and economic and social well-being should be considered. In a lot of states which allow the life of the mother to prevail over the life of the embryo and foetus, it still seems to be a matter of life and death as the condition for allowing an abortion. Unsurprisingly, since these same states rarely offer pre- and post-natal health care, have very low benefits and a weak social welfare state, it is evident that the life of the mother and child are not their true concern at all.
One thing that I haven’t heard discussed by the right in the US was whether this child would be able to survive a full-term pregnancy. Even more so, was whether she should even be forced to try to do so. When the life of a child is endangered by your foetal fetishism, your bullshite that you are concerned with the life of a child is revealed openly. Is this child’s life of no importance compared to the gestating foetus she is being forced to carry to term? How can a 10 year old (whom most of these fools do not realise they can get pregnant) be forced to carry a child because of your need to demonstrate male power over women/girls to make men feel more empowered?
Don’t worry, you have no power in your own life because of the nature of the capitalist system, but be reassured, you still have power over women, people of colour, disabled people and LGBT+ people. You are one step on the social ladder above another group of people. That the social, political and economic oppression that is part and parcel of this society is used to make some people who have lost a little power feel a bit better is a codification of oppression used by the ruling class to play divide and rule amongst the exploited and oppressed.
This 10 year old child who had experienced rape, now has had her horrific experience splashed all over the media and denied by ignorant politicians. It is disgusting. What this situation does demonstrate is that there must never be conditions made and explanations provided for why you want an abortion. This must be a fundamental demand of the pro-choice movement and we must support this demand. We can see what happens when this does not happen. The right-wing and fundamentalist Christians will play divide and rule, we never should need to offer explanations of why we choose if we have children or not, when and how many. This is a right of bodily autonomy and we do know that banning abortion doesn’t end abortions, what it does is make abortions unsafe and it increases the possibility of maternal death (and let’s not forget criminalisation).
Reproductive Justice
What we must understand in our fightback on abortion rights, is that it must be done in the context of the struggle for reproductive justice. The failure of the Democratic Party and mainstream feminism to understand the different historical experiences of people of colour, of people with low incomes (e.g., women are often trapped in part-time work due to social reproduction responsibilities, people of colour who have lower incomes due to racism), of disabled people, and LGBT+ people means that the struggles around contraceptives, abortion and sterilisation did not take into account the different needs of different groups of people in our society.
Moreover, we need to remember that being pro-choice means that we support the right of those that can get pregnant to choose if, when and how many children they have. Overall, we need to understand the different constraints that people that can get pregnant operate under. Constraints are economic, cultural, religious, and societal. People face a whole host of situations that are beyond their control which impact on their decisions to have children; economic issues are only one area. The fact that women are more dependent on welfare benefits, means that they are concerned whether they can support their children, and this can play a very important role in your choice. Historical experience and the impact of racism, disablism, homophobia and transphobia limits choice. Different cultural and religious beliefs relating to the rights of women impact on the choices you perceive yourself as having. These constraints operate in the societies we live and if we refuse to recognise the impact of racism, disablism, class, homophobia and transphobia we are removing people from a discussion about their most basic right; that is the right to bodily autonomy.
Access to general healthcare and reproductive healthcare differs substantially and is dependent upon your class. Access to healthcare being tied to employment as it has been in the US means that there are those that are in work but not eligible for healthcare (e.g., part-time workers, precarious workers). As such, preventative healthcare is far rarer for those with low incomes. Access to Medicaid does not necessarily mean that you can access reproductive health care.
Eugenics
The power of the eugenics movement in the US and its linkage to the birth control movement led to the differential treatment of those that can get pregnant. “Middle” income working class white women and wealthy white women were prevented from having abortions and could not get sterilisations without their husbands’ permission. In the case of poor working-class women, disabled women and women of colour, the role of eugenics had a very different effect. Since they were not seen as perfect white members of the human race that was wanted to breed by the ruling class, their fertility was often undermined.
This led to forced use of contraceptives (sometimes tied to receipt of welfare benefits and/or release from prison) as these women are considered a drain on civilised white society. People that had children that might be dependent on welfare benefits were encouraged to not have children, forced eugenics sterilisation was used against disabled people, against those with lower incomes and the “uneducated”, against women that did not conform to societal notions of how women should behave, such as sex workers and convicted offenders.
Forced sterilisation in the US was a practice that began in the early 20th century, it was initially targeted at disabled people, but also impacted upon poor women who came under control of welfare boards from the 1940s to the 1970s. Under the Nixon Administration (late 60s-early 70s) Medicaid funded sterilisations targeted especially people of colour during the second wave of forced and coerced sterilisations as these were conducted as part of accessing healthcare as part of the welfare state. It’s estimated that anywhere from 100,000-150,000 women were sterilised in this period. Forced or coerced sterilisation of prisoners still exists today in the US and is often directed at people in prison as a condition for their release or reducing sentences.
Elizabeth Raterman states:
“In May 2017, a Tennessee judge signed a standing order allowing inmates in White County to receive jail credit if they underwent either a vasectomy for males or a Nexplanon implant for females. Thirty-two women and thirty-eight men underwent sterilization during the three months Judge Benningfield’s order was in effect. Though Tennessee later introduced a bill that would forbid judges from approving a reduced sentence if it is conditioned upon sterilization, other states are not responding with similar legislation. In February 2018, an Oklahoma woman, who was a prior drug addict, received a shorter sentence for a federal counterfeiting offense after undergoing surgery to prevent further pregnancies.”
Rarely are disabled people included in discussions of reproductive rights. This is an example of the influence of eugenics that has been normalised as well as a decision on eugenics sterilisation of the Supreme Court of the United States called Buck vs Bell (1927). Buck vs Bell is one of those notorious decisions that should be raised along with Plessey vs Ferguson as appalling decisions by the SCOTUS. This decision allowed that the compulsory eugenic sterilisation of the “unfit” and “feeble” (including those with intellectually impairments) in Virginia was not a violation of the Due Process Clause of the 14th Amendment of the Constitution for those with impairments. It led to eugenics sterilisation laws being passed in most states in the US at the time. This decision has never been overturned or ameliorated by the SCOTUS (Skinner vs Oklahoma in 1942 related to men in prison and forced sterilisation to ensure release).
This continues today. For disabled women, there is active discouragement from having children as though because you have an impairment, you are either incapable or unqualified to be a parent. Under the guise of disabled people’s dependence on their families and state benefits and their social exclusion (which we know is societal) from society, they are often viewed as unable to understand sex and the responsibilities of being a parent. Under guardianship laws, disabled people can still be sterilised in 31 US states and Washington DC.
Compulsive sterilisation of disabled, poor and women of colour was legal in the US and part of social policy. This policy was essential to ensure the genocide of Native American women. In the US colony of Puerto Rico, not only was the early versions of the birth control pill tested on women, but women were 35% more likely to be sterilised compared to women on the mainland in 1968. This was official policy of the US government.
Class, race and gender and access to healthcare
The fact that the Hyde Amendment is still in place after the overturn of Roe and Casey is telling. Even in states that have banned abortion or are in the process of banning or curtailing accessibility, this poisonous rider to budgetary bills still is relevant. The states that have protected abortion right often exceeded the requirements of the Hyde Amendment allowing Medicaid funded abortions already. So even in the current climate where pregnant people are losing their rights to bodily autonomy, they still have the Hyde Amendment to deal with.
Most importantly, the Hyde Amendment targeted the poorest members of the working class. (women often predominate part-time labour and in the US, have no access to holidays and sick days) It targeted people of colour who because of racism often work in sectors with lower wages and have lower incomes., targeted people dependent upon Federal provision of healthcare, (e.g., Native Americans, veterans, people in the armed forces, and federal employees). In essence, the Hyde Amendment meant that even though abortion was a legal right, accessing that right depended on state law and Medicaid provision, income and savings.
Maternal death rates in the US are rising and there are distinct differences between the numbers of women of colour and white women. According to the Maternal Health Task Force,
“The most notable disparity in mortality rates in the U.S. is defined by race: Black women die at a rate that ranges from three to four times the rate of their white counterparts—41 deaths per 100,000 live births among black women versus 13 deaths per 100,000 live births among white women as of 2010; this difference in risk has remained unchanged for the past six decades. American Indian and Alaskan Native women also fare worse than white women with approximately twice as many pregnancy-related deaths per 100,000 live births. Women of color tend to have poorer access to high quality reproductive health information and services than white women, are discriminated against in the healthcare system and experience higher rates of disrespect and abuse. Furthermore, there is evidence suggesting that the stress associated with situational experiences of racial discrimination can increase the risk of negative perinatal outcomes including preterm birth and infant death for Black women. Maternal mortality ratios also vary significantly by socioeconomic status and geography. Women living in poverty and women in certain states experience significantly higher MMRs than the national average.”
These results are replicated in a report by the Centers for Disease Control and Prevention (2020):
“This report updates a previous one that showed maternal mortality rates for 2018 and 2019 (2). In 2020, 861 women were identified as having died of maternal causes in the United States, compared with 754 in 2019 (3). The maternal mortality rate for 2020 was 23.8 deaths per 100,000 live births compared with a rate of 20.1 in 2019 (Table).
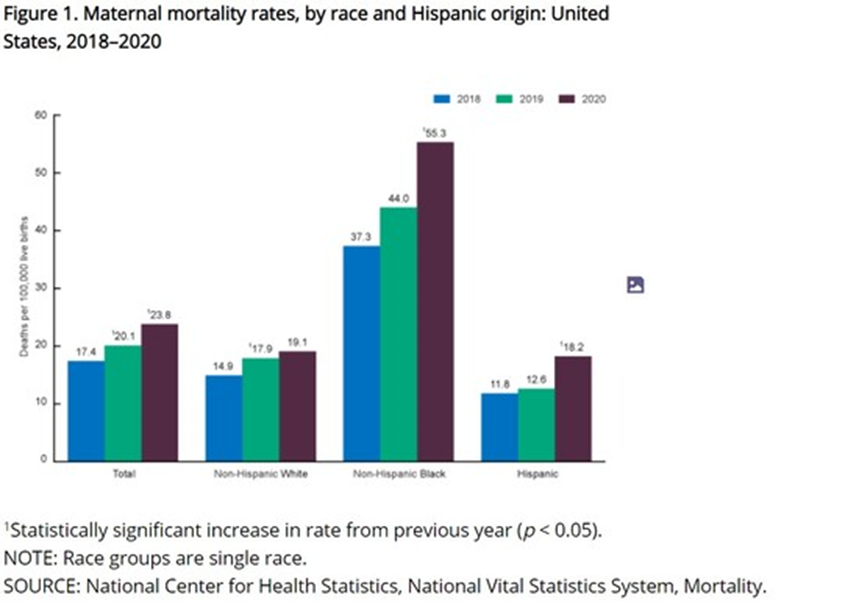
In 2020, the maternal mortality rate for non-Hispanic Black women was 55.3 deaths per 100,000 live births, 2.9 times the rate for non-Hispanic White women (19.1) (Figure 1 and Table). Rates for non-Hispanic Black women were significantly higher than rates for non-Hispanic White and Hispanic women. The increases from 2019 to 2020 for non-Hispanic Black and Hispanic women were significant. The observed increase from 2019 to 2020 for non-Hispanic White women was not significant.
Rates increased with maternal age. Rates in 2020 were 13.8 deaths per 100,000 live births for women under age 25, 22.8 for those aged 25–39, and 107.9 for those aged 40 and over (Figure 2 and Table). The rate for women aged 40 and over was 7.8 times higher than the rate for women under age 25. Differences in the rates between age groups were statistically significant. Among age groups, the increase in the rates between 2019 and 2020 for women aged 25–39 and 40 and over were statistically significant.”
As such, when we discuss access to abortion or reproductive healthcare (e.g., pap/cervical smears, a wide variety of contraceptives, sterilisation, prenatal and post-natal healthcare, breast cancer scans, fibroids, endometriosis, etc), we must understand that this is a class issue and it is also an issue for people oppressed by racism, by being disabled by society, and being LGBT+.
It is not only women that can get pregnant, non-binary people and trans men can also get pregnant, we need to ensure their access to abortion as well as to various types of contraceptives. After decades of struggle, forced sterilisation of trans and intersex people was declared torture by the World Health Organisation in 2013 and declared illegal by the European Court of Human Rights in 2017. The picture to the left shows countries that required sterilisation for trans people to transition (in orange), where it was not required (in blue), where there was no law on it at all (green).
Obviously, this is not only a problem in the US. However, what happens in the US affects other countries for a variety of reasons; Foreign aid which addresses reproductive healthcare will be impacted . Further the shift toward the hard-right in the US legitimises and normalises violations of guaranteed human rights for those that can get pregnant across the world.
According to the Center for Reproductive Rights:
“970 million women, representing 59% of women of reproductive age, live in countries that broadly allow abortion. While a majority of women live in countries where they can exercise their right to abortion, 41 percent of women live under restrictive laws. The inability to access safe and legal abortion care impacts 700 million women of reproductive age. According to the World Health Organization, 23,000 women die of unsafe abortion each year and tens of thousands more experience significant health complications. Legal restrictions on abortion do not result in fewer abortions, instead they compel women to risk their lives and health by seeking out unsafe abortion care. […] 90 million women (5% of the world’s population) live in countries where women are completely prohibited from having an abortion.“
The attack by the hard-right on bodily autonomy for those that can get pregnant, for those fighting against homophobia and transphobia is happening in other states in the world. The overturn of Roe and the upcoming attack on the right of privacy (ignore the denials, if abortion is not found in the constitution, neither is the right to privacy) will further these attacks in other countries and will legitimise the attacks already underway in countries like Poland, Hungary and Russia, among others.
The Danger of Criminalisation
Given that the fertilised egg is being treated as a child in Ohio (and probably in other states), another issue that we need to be concerned with is miscarriage and criminalisation of those that have a miscarriage. If you miscarry an embryo or a foetus given the sanctity of a fertilised egg, embryo or foetus, the nature of the miscarriage could endanger you criminally. Laws passed to protect violence against women can be used against those who miscarry a foetus. In many countries where abortion is criminalised, women that miscarry can be charged with manslaughter or even murder.
Black people have a higher rate of miscarriage and face poverty, structural and institutional racism and criminalisation as well as predispositions to certain health conditions (i.e., sickle cell anaemia, diabetes and high blood pressure), medical treatment and support for those that miscarry should be a priority. Instead of support and recognising the pain of those that have a miscarriage, women may face criminalisation due to racism, and the criminalisation of poverty.
In El Salvador, abortion is completely banned. Further, those that have miscarriages or medical emergencies relating to a pregnancy routinely face charges of aggravated homicide.
“Hundreds of Salvadoran women have been charged with abortion or aggravated homicide in the past 25 years. Under the 1997 penal code, the crime of abortion carries a prison sentence of two to eight years; aggravated homicide, 30 to 50 years.”
The debate over abortion in the US has also led to criminalisation of women that have miscarried. They are criminalised for taking drugs (often those that have no impact on foetus) during pregnancy seen as child abuse; a few have been charged for accidentally falling during pregnancy. Women have been prosecuted for abusing a corpse following a miscarriage. In 2021 in Oklahoma, Britney Poolaw was convicted for second degree manslaughter for miscarrying a 17 week old foetus due to taking methamphetamine during pregnancy. This happened despite medical professionals’ opinion that methamphetamine does not cause the birth defects that led to the miscarriage; she was convicted and sentenced to 4 years in jail. According to Megan Carpentier quoting Dana Sussman of the National Advocates for Pregnant Women:
“Statistics developed by the NAPW show that cases like Poolaw’s — in which women are prosecuted for miscarriages or stillbirths that the state decides they caused, and/or for drug use during pregnancy— are increasingly more common. Since the legalization of abortion in 1973, a total of 1,600 women in the United States were prosecuted for actions during their pregnancies, the NAPW says; 1,200 of those women were prosecuted after 2006.
Oklahoma, with 57 such cases documented since 2006 and only nine before, is fourth in the nation for such prosecutions. (Alabama accounts for 500 of the 1,200 cases since 2006, making it the state most likely to prosecute women for actions during their pregnancies, followed by South Carolina and Tennessee.)”
Conclusion
The situation we are experiencing is extremely dangerous and does not only affect women. This is always the case when the hard-right strengthens its political power. The history of sterilisation abuse in the US is not just history; understanding the combined impacts of racism, disablism, homophobia, transphobia and class is essential if we are actually going to have a coherent fightback against the upcoming attack on civil rights that have been struggled over for decades in the US.
All movements of the oppressed need to be standing together and we must not allow the mainstream feminist movement to remain in control of this struggle; their failures to understand that their history and struggle are not necessarily the struggle of all women. We have different histories and current experiences that this movement simply refuses to acknowledge or understand. Nor should we trust the Democratic Party to control this fight; they have failed horribly over the 5 decades since Roe vs Wade was decided; neither eliminating the Hyde Amendment, their inability to codify the right of abortion in law, never ensuring that this right was actually accessible to all those that needed an abortion. It was evident that Roe was going to be overturned from the oral arguments at the SCOTUS and they did nothing. Biden’s proclamation is meaningless and offers nothing to those living in states where not only abortion is being eliminated. If the Texas Law about helping someone get an abortion is ruled to be legal; the ability to travel across state lines could be hindered. Will people need to prove they are not pregnant to get in a cab, on a train or on a plane. The Polish government’s attempt to create a pregnancy and miscarriage registry is extremely dangerous and let’s be real, can you not imagine that this will be adopted in states that ban abortion?
Moreover, we need to understand that this is a struggle that goes well beyond the US. We need to stand in solidarity with people in the US whose bodily autonomy is threatened, just as people in the US need to stand with others outside the US facing the same. That is the nature of solidarity.
Source > Daily Kos
Art Book Review Books Campism Capitalism China Climate Emergency Conservative Government Conservative Party COVID-19 Creeping Fascism Economics EcoSocialism Elections Europe Far-Right Fascism Film Film Review Fourth International France Gaza History Imperialism Iran Israel Italy Keir Starmer Labour Party Long Read Marxism Marxist Theory Migrants Palestine pandemic Police Protest Russia Solidarity Statement Trade Unionism Trans*Mission Ukraine United States of America War